要旨
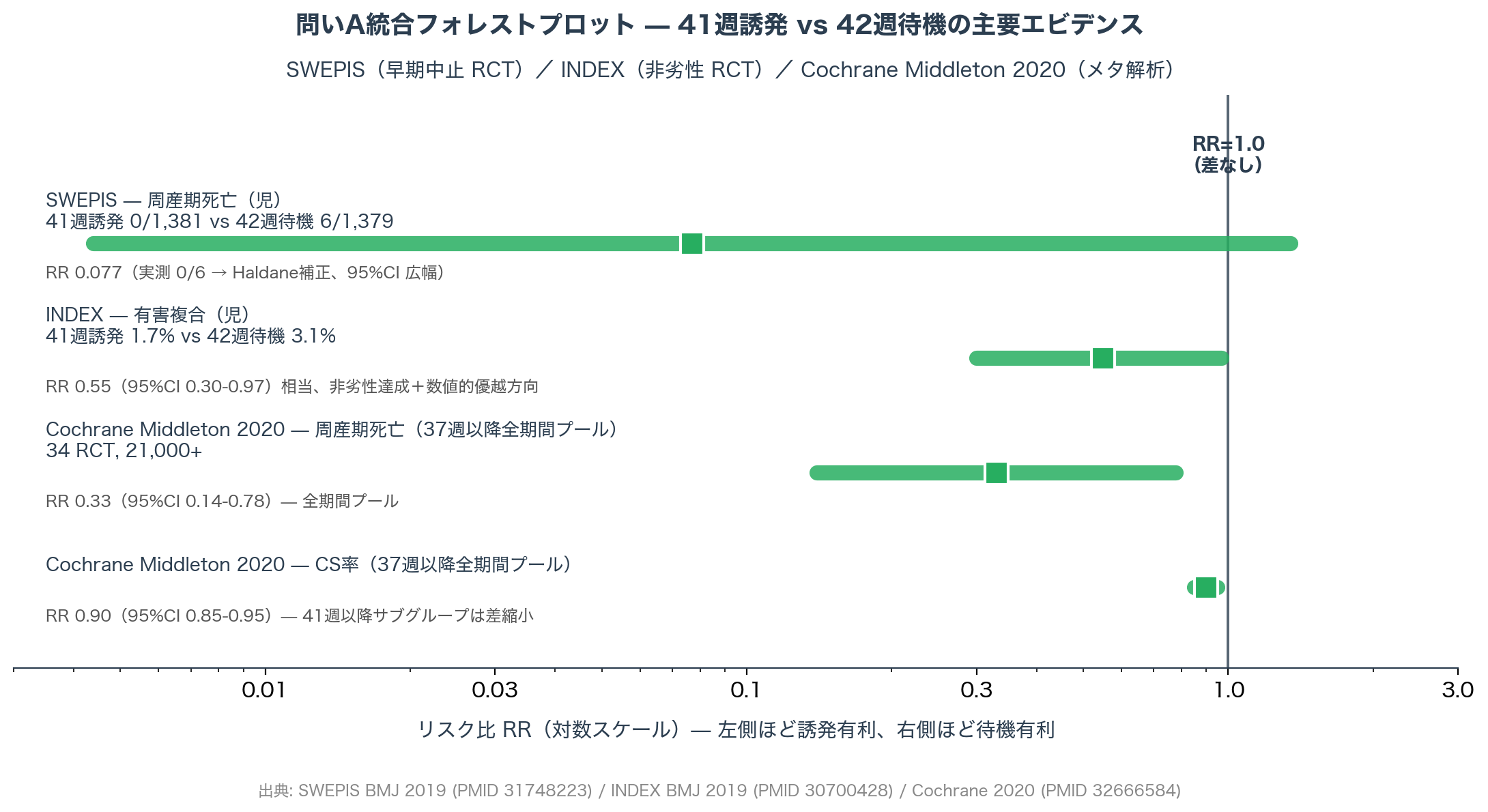
本稿は、ARRIVE 以降 8 年のエビデンスを「39 週誘発」と「41 週超え管理」の独立した 2 問に分解して再構築する。問い A(41 週超え管理)は SWEPIS / INDEX / Cochrane Middleton 2020、加えて Place K 2024 AOGS (NFOG 公式機関誌掲載 RCT、JSOG 2026 CQ409 reference #13) を統合。問い B(39 週誘発)は ARRIVE / Hong 2023 サブグループ・post-ARRIVE 4 研究(Jelks / Gilroy / Wood / Nethery)・Fitzgerald 2023 のコスト効果・Lindquist / Yisma / Werner の causal inference 3 研究まで体系化し、JSOG 2026 CQ409 原文と国際 GL 6 者の散らばりを 4 軸で整理する。
本論の要点
記事本文(数値解析・原典精読・国内実装の論点)は note 医師向けマガジンで配信しています。本ページでは、論点の構造と図表アーカイブのみを公開しています。
本稿が踏み込む 5 つの論点
- 「39 週誘発」と「41 週誘発」は別の問いである — この区別なしに議論すると論点が崩れる。2 問に分け、それぞれの決着度を判定する。
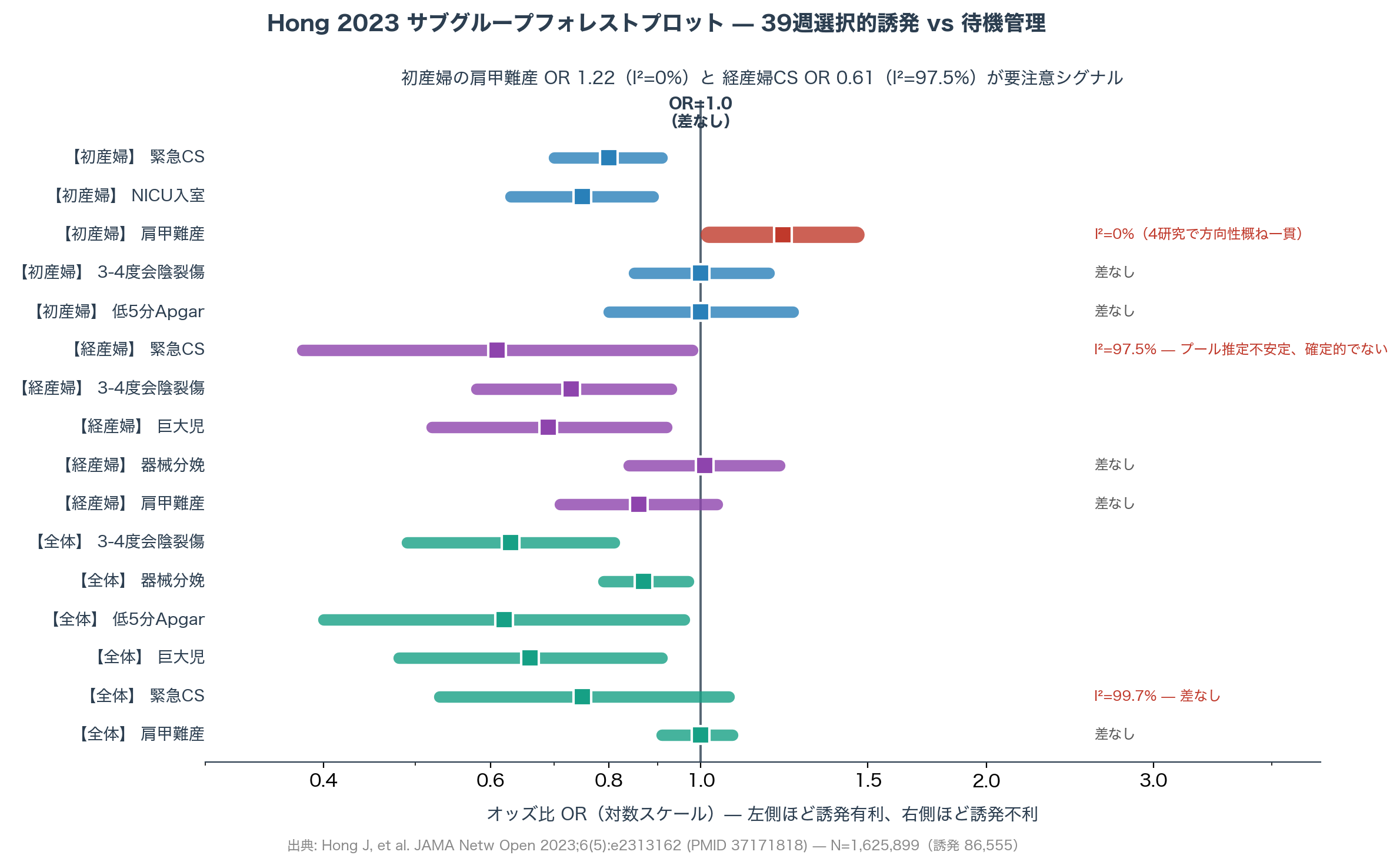
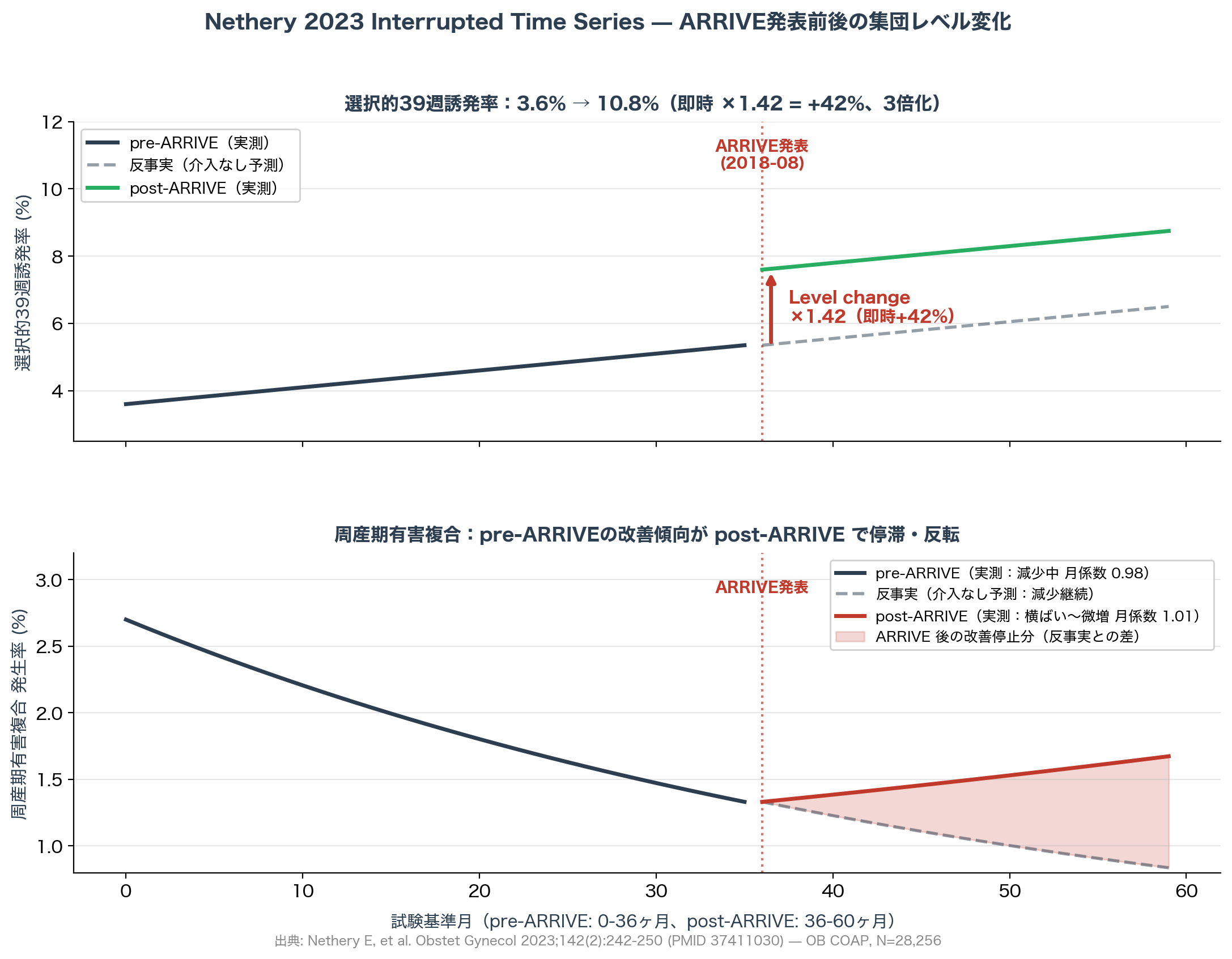
- ARRIVE の外的妥当性危機 — 提示同意率 27%(Mallett 2020)、post-ARRIVE 4 研究(Jelks / Gilroy / Wood / Nethery)の実臨床データ、Hong 2023 メタ解析の経産婦含む最新統合まで踏み込む。
- コスト効果の実像 — Hersh 2019 / Einerson 2020 / Fitzgerald 2023 を IMRAD で並列分析。米国閾値でも全体集団ではギリギリ(Hersh)、子宮口開大度別では結論が割れる(Fitzgerald)。
- 長期神経発達への懸念は払拭されたか — Sotiriadis 警告(MacKay の「40-41 週が最適」観察)に対し、Lindquist 2022 / Yisma 2021 / Werner 2020 が causal inference で直接検証。3 本とも 39 週誘発の悪影響を支持しなかった。
- JSOG 2026 vs ACOG / NICE / WHO / スウェーデン / フィンランド (Place K RCT) を主要 4 軸で整理 — 引用エビデンス基盤・政策フレームワーク・対象集団・改訂年の 4 軸で 6 者の散らばりを整理する。
図表アーカイブ


本文をお読みになるには
本論文の原典精読・統合解析・国際 GL 比較は note 医師向けマガジンで配信しています。引用論文 25 本以上、有料閲覧 70,962 字、返金可。
主要参考文献
問い A(Post-term 管理)
- Wennerholm UB, et al. Induction of labour at 41 weeks versus expectant management and induction of labour at 42 weeks (SWEPIS). BMJ. 2019;367:l6131. PMID: 31748223
- Keulen JK, et al. Induction of labour at 41 weeks versus expectant management until 42 weeks (INDEX). BMJ. 2019;364:l344. PMID: 30786997
- Middleton P, et al. Induction of labour at or beyond 37 weeks' gestation. Cochrane Database Syst Rev. 2020;(7):CD004945. PMID: 32666584
- Place K, et al. Labor induction at 41+0 gestational weeks or expectant management for the nulliparous woman: The Finnish randomized controlled multicenter trial. Acta Obstet Gynecol Scand. 2024;103(3):505-511. PMID: 38112629
問い B(39 週誘発)
- Grobman WA, et al. Labor Induction versus Expectant Management in Low-Risk Nulliparous Women (ARRIVE). N Engl J Med. 2018;379(6):513-523. PMID: 30089070
- Sotiriadis A, et al. Maternal and perinatal outcomes after elective induction of labor at 39 weeks: a meta-analysis. Ultrasound Obstet Gynecol. 2019;53(1):26-35. PMID: 30298532
- Hong J, et al. Elective induction of labor at 39 weeks: systematic review and meta-analysis. JAMA Netw Open. 2023;6(5):e2313162. PMID: 37171818
- Mallett G, et al. Characteristics Associated With Consent and Reasons for Declining in a Randomized Trial in Pregnancy (ARRIVE). Obstet Gynecol. 2020;136(4):731-737. PMID: 32925629
post-ARRIVE リアルワールド観察研究
- Gilroy LC, et al. Changes in obstetrical practices and pregnancy outcomes following the ARRIVE trial. Am J Obstet Gynecol. 2022;226(5):716.e1-716.e12. PMID: 35139334
- Wood R, et al. Rates of Induction of Labor at 39 Weeks and Cesarean Delivery Following Publication of the ARRIVE Trial. JAMA Netw Open. 2023;6(8):e2328274. PMID: 37561464
- Nethery E, et al. Effects of the ARRIVE Trial on Elective Induction and Obstetric Outcomes in Term Nulliparous Patients. Obstet Gynecol. 2023;142(2):242-250. PMID: 37411030
コスト効果・長期神経発達・ACOG 現行
- Hersh AR, et al. Induction of labor at 39 weeks: cost-effectiveness analysis. Am J Obstet Gynecol. 2019;220(6):590.e1-590.e10. PMID: 30768934
- Fitzgerald AC, Kaimal AJ, Little SE. Cost-effectiveness of induction of labor at 39 weeks by cervical examination. Am J Obstet Gynecol. 2023;229(2):162.e1-162.e9.
- Lindquist A, et al. Developmental outcomes for children after elective birth at 39 weeks' gestation. JAMA Pediatr. 2022;176(7):654-663. PMID: 35532925
- Yisma E, et al. Elective labor induction vs expectant management of pregnant women at term and children's educational outcomes at 8 years of age. Ultrasound Obstet Gynecol. 2021;58(1):99-104. PMID: 33030765
- Werner EF, et al. Association of term labor induction vs expectant management with child academic outcomes. JAMA Netw Open. 2020;3(4):e202503. PMID: 32275323
- American College of Obstetricians and Gynecologists. Management of Full-Term Nulliparous Individuals Without a Medical Indication for Delivery: ACOG Clinical Practice Update. Obstet Gynecol. 2025;145(1):e45-e50. PMID: 39513607
ガイドライン
- NICE Guideline [NG207]: Inducing labour. 2021.
- World Health Organization. WHO recommendations on induction of labour, at or beyond term. Geneva: WHO; 2022.
- 日本産科婦人科学会/日本産婦人科医会. 産婦人科診療ガイドライン — 産科編 2026. CQ409.
- Nationellt system för kunskapsstyrning (Sweden). Riktlinje för handläggning i graviditetsvecka 41. 2021.